
What do psych hospitals record on their Q15 sheets?
We analyzed the more than 300 survey responses collected by the American Psychiatric Nurses Association when they asked participants “What issues are documented during a safety check and how are they documented?”
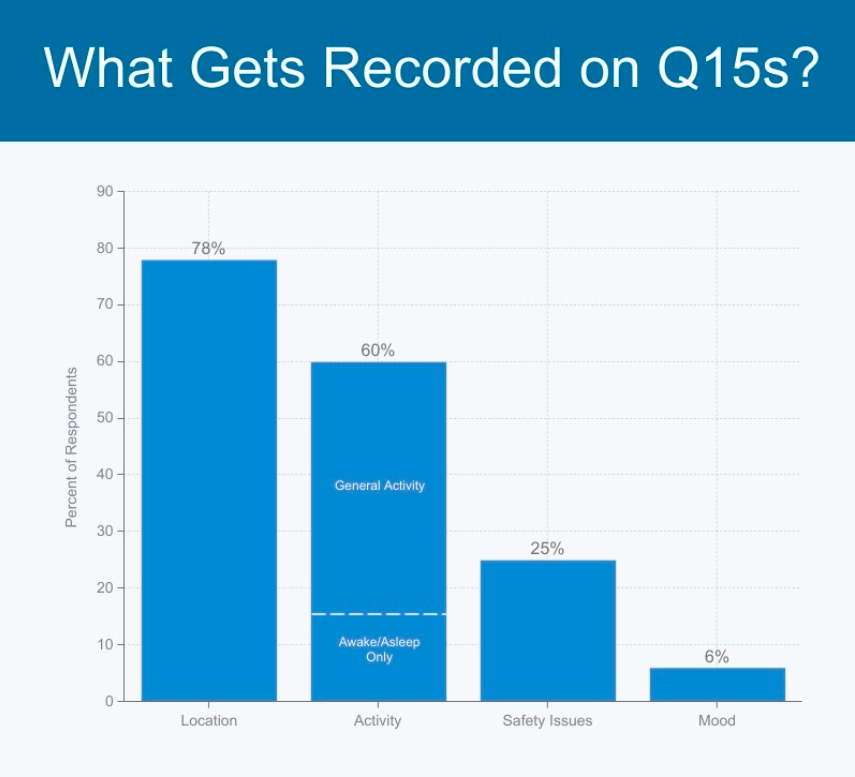
We found that the majority of documented issues fit into the following four areas: Patient Location, Patient Activity, Safety Issues related to the patient or environment, and Patient’s Mood. The accompanying chart summarizes the percentage of respondents who highlighted each of these areas.
One additional takeaway: Q15s can take a long time if there are many patients and the rounding system (paper or digital) is inefficient. One respondent stated: “We document where and what the patient is doing using a paper document. Will soon have the option of using the computer but will continue on paper because the computer option is too cumbersome.”
Using a digital rounding system alongside an existing EHR is a great way to improve Q15 quality while gaining efficiency. Digital rounding is more efficient than an EHR from the documentation standpoint (simple mobile app vs. 20 computer clicks per observations). And digital rounding is more efficient than paper rounding from a logistics standpoint (no more binders, folders, printing, scanning, uploading, etc.)
In all cases, whether upgrading from paper or from an EHR, the simplicity and validation gained by using a digital rounding platform like VisibleHand will bring a unit to 100% compliance within days.
A sample of responses directly from the APNA survey: (Visit APNA for all 300+ responses)
- Each patient has a hand written check sheet which lists patient’s location, behavior, and presence or absence of visible contraband is documented.
- Location of patient, who is with them, what are they doing at time
- Patient location and activity. This process is still on paper. Staff carry a clipboard and document concurrently.
- Activity at present is documented by computer clicks in flow columns on computer and on hard copy sheets that technicians carry.
- What the person is doing (sitting, standing, showering, etc) and their location (room, day room, bathroom etc).
- Location of patient and activity of patient on a paper form with boxes for every 15 minutes - use codes in the boxes to indicate location and activity
- Activities of the patient including respiration when sleeping.
- Location of patient, if they are sleeping, in restraints, lock door checks, 1:1, staff signature, times, date shift.
- Brief behavior codes on a check sheet and for 15/30/60 min checks. Broset Scale each shift all points are filled out for each patient
- A check off on the electronic record indication 15 minute rounds conducted for safety and a paper 15 minute check off which notes location of patient only
- Rooms are checked, locks are checked, looks for hazards (water on floor, obstructed exits, etc.)
- We have a board with each patient name, the safety or precaution status i.e. suicide precautions violence precautions, fall precautions, seizure precautions, the staff must see the patient and mark down on the board where they are what they are doing
- We document where and what the patient is doing using a paper document. Will soon have the option of using the computer but will continue on paper because the computer option is too cumbersome.
- The patient’s location and activity/ behavior, with the level of detail depending on the acuity
- Location of the patient, that the "sharps" have been accounted for, and other environmental issues have been checked - there are specific areas to initial on a spread sheet.
- Patient whereabouts are documented on a flow sheet to include location and if it is at night, then the sleep status is also included.
- Are doors locked that are not in use? Scan empty rooms for sharp objects, that patient is alive, safe & breathing - documented with a checkbox method on clipboard
- Patient safety checks/observations are only whether patient is awake or sleeping and breathing. Documentation is on a paper sheet that has staff signatures and all patients listed with a photo, room assignment and observation level. Fall risk is indicated on this form as well as elopement risk.
- Location (Day Rm, Group Rm, Bedrm), Behavior (Calm, Agitated) Actions (Talking, Sleeping) Check sheet w/ codes (DR, C, T) (Day Rm, Calm, Talking) Staff sign the sheet and initial each entry.
- Any reported near miss, or error, or unsafe environmental issue, practice, or process is documented and followed up with action plan by a combination of the unit/program leadership and the system quality/safety committee.
- If the patient is or is not suicidal (if patient is suicidal then they will be asked to come to dayroom for closer observation) and if they can agree to tell staff if they do become suicidal
- Documentation is by a check mark on a form and the location. The CNA's are primarily responsible for safety checks. If there is an issue, they report to the charge nurse.
- Our unit uses a safety check "matrix" that includes pt's name w/ small boxes indicating 1/2 hr time intervals. We use pre-set initials to indicate what pt is doing or where pt is at that time; i.e., LR (in living room), MD (w/ doctor), BR (in bathroom), etc.
- For patient safety checks, patient exact location is documented. For environmental safety checks each pt room is observed for potential hazards, contraband and repair needs.
- #1 location of patient, and at night, whether or not the patient is sleeping; #2 presence and description of any contraband found; #3 doors that are to be locked are locked, hardware working properly, pagers and alarms working, intercom system working...etc. If any repairs are indicated, a work order is completed.
- For the 15 min checks on each pt we have one sheet with every pt's name on it. Codes are used to indicate where the pt was and what their behavior was at the time. For the checks done once a shift a different check sheet is used that includes whether or not doors are locked, wet towels removed from bathrooms, staff wearing name pins etc
- We document where the patient is located when we do the safety check. We document if someone signs out a sharp item, which is an item that could be used as a weapon to harm themselves or others examples would be a portable DVD player, a razor which needs to be used in staff supervision and turned back in immediately. Cds music or DVD’s, portable CD players, notebooks with wire binders etc.
- For 30 min checks we have a one page grid with times across the top and patients names down the side. We document their location on each safety check. For 15 min. checks there is an individual form for each patient; staff document location and initial each time.
- Presence medical equipment or other potentially "unsafe" items, e.g. call light cord; restraint gurney is checked for readiness; doors locked; documented on mental health tech's flow sheet
- We decided to take out behaviors from our checks document so we document location. The only behavior is sleep. We decided no matter where they are if they are sleeping that is important information. So Z is for sleeping. Otherwise it is location such as room, hallway, dayroom, dining room, and group.